


Congenital syphilis is a multisystem infection caused by Treponema pallidum and is transmitted to the fetus via the placenta. Early signs are characteristic skin lesions, lymphadenopathy, hepatosplenomegaly, growth and weight faltering (formerly failure to thrive), blood-stained nasal discharge, perioral fissures, meningitis, choroiditis, hydrocephalus, seizures, intellectual disability, osteochondritis, and pseudoparalysis (Parrot atrophy of newborn). Later signs are gummatous ulcers, periosteal lesions, paresis, tabes, optic atrophy, interstitial keratitis, sensorineural deafness, and dental deformities. Diagnosis is by history and physical examination, confirmed by microscopy or serology. Treatment is penicillin.
(See also Syphilis in adults and Overview of Neonatal Infections.)
Overall risk of transplacental infection of the fetus is approximately 60 to 100%, and likelihood is increased during the second half of the pregnancy. Untreated primary or secondary syphilis in the mother usually is transmitted to the fetus, but latent or tertiary syphilis is transmitted in approximately 7 to 40% of cases (1). Untreated syphilis in pregnancy is also associated with preterm delivery and a significant risk of stillbirth and neonatal death.
The incidence of congenital syphilis has increased 755% in the United States from 2012 to 2021 (2). In the United States in 2023, over 3800 congenital syphilis cases were reported, including 279 fetal, neonatal, and infant deaths (3). Inadequate treatment and lack of timely testing contribute to disparities in congenital syphilis rates by geography, race, and ethnicity in the United States (4).
Worldwide in 2022, an estimated 700,000 cases of congenital syphilis were reported (5).
In infected neonates, clinical manifestations of syphilis are classified as early congenital (ie, birth through age 2 years) and late congenital (ie, after age 2 years).
General references
1. Committee on Infectious Diseases, American Academy of Pediatrics: Syphilis in Red Book: 2024–2027 Report of the Committee on Infectious Diseases, ed. 33, edited by Kimberlin DW, Banerjee R, Barnett ED, Lynfield R, and Sawyer MH. Itasca, American Academy of Pediatrics, 2024.
2. McDonald R, O'Callaghan K, Torrone E, et al. Vital Signs: Missed Opportunities for Preventing Congenital Syphilis - United States, 2022. MMWR Morb Mortal Wkly Rep. 2023;72(46):1269-1274. Published 2023 Nov 17. doi:10.15585/mmwr.mm7246e1
3. Centers for Disease Control and Prevention (CDC): Sexually Transmitted Infections Surveillance, 2023.
4. McDonald R, O'Callaghan K, Torrone E, et al. Vital Signs: Missed Opportunities for Preventing Congenital Syphilis - United States, 2022. MMWR Morb Mortal Wkly Rep. 2023;72(46):1269-1274. Published 2023 Nov 17. doi:10.15585/mmwr.mm7246e1
5. World Health Organization (WHO): Data on syphilis. Accessed November 20, 2024.
Symptoms and Signs of Congenital Syphilis
Many patients are asymptomatic at birth.
Early congenital syphilis commonly manifests during the first 3 months of life. Clinical manifestations include characteristic vesiculobullous eruptions or a macular, copper-colored rash on the palms and soles, which can be lighter or darker than the surrounding skin. Other skin findings include papular lesions around the nose and mouth and in the diaper area, as well as petechial lesions. Generalized lymphadenopathy, thrombocytopenia, hemolytic anemia, and hepatosplenomegaly often occur. The infant may have growth and weight faltering and a characteristic mucopurulent or blood-stained nasal discharge causing snuffles.
A few infants develop meningitis, choroiditis, hydrocephalus, or seizures, and others may be intellectually disabled.
Within the first 8 months of life, osteochondritis (chondroepiphysitis), especially of the long bones and ribs, may cause pseudoparalysis of the limbs with characteristic radiologic changes in the bones.


Late congenital syphilis typically manifests after 2 years of life and causes gummatous ulcers that tend to involve the nose, septum, and hard palate and periosteal lesions that result in saber shins and bossing of the frontal and parietal bones. Intellectual disability, juvenile paresis, and tabes dorsalis may develop.
Optic atrophy, sometimes leading to blindness, may occur. Interstitial keratitis, the most common eye lesion, frequently recurs, often resulting in corneal scarring.
Sensorineural deafness, which is often progressive, may appear at any age.
Hutchinson incisors, mulberry molars, perioral fissures (rhagades), and maldevelopment of the maxilla resulting in “bulldog” facies are characteristic, if infrequent, sequelae.


Osteoperiostitis of the tibia leads to characteristic saber shins in this patient with congenital syphilis.
Image courtesy of Robert Sumpter via the Public Health Image Library of the Centers for Disease Control and Prevention.


Interstitial keratitis manifests with varying degrees of corneal opacification and neovascularization. The neovascularization appears as the faint, pink areas in the peripheral cornea from the 11 o'clock to the 1 o'clock position.
© Springer Science+Business Media


This photo shows triangular shaped deformity of right upper and left lower incisors caused by congenital syphilis.
Image courtesy of Robert E. Sumpter via the Public Health Image Library of the Centers for Disease Control and Prevention.
Osteoperiostitis of the tibia leads to characteristic saber shins in this patient with congenital syphilis.
Image courtesy of Robert Sumpter via the Public Health Image Library of the Centers for Disease Control and Prevention.
Interstitial keratitis manifests with varying degrees of corneal opacification and neovascularization. The neovascularization appears as the faint, pink areas in the peripheral cornea from the 11 o'clock to the 1 o'clock position.
© Springer Science+Business Media
This photo shows triangular shaped deformity of right upper and left lower incisors caused by congenital syphilis.
Image courtesy of Robert E. Sumpter via the Public Health Image Library of the Centers for Disease Control and Prevention.
Diagnosis of Congenital Syphilis
Early congenital syphilis: Physical examination; darkfield microscopy or staining of lesions, placenta, or umbilical cord; serologic testing of mother and neonate; possibly cerebrospinal fluid (CSF) analysis
Late congenital syphilis: Physical examination, serologic testing of mother and child
Early congenital syphilis
Diagnosis of early congenital syphilis is usually suspected based on maternal serologic testing, which is routinely performed early in pregnancy, and repeated in the third trimester and at delivery if risk factors are present. Neonates of mothers with serologic evidence of syphilis should have a thorough examination, darkfield microscopy or immunofluorescent staining of any skin or mucosal lesions, and a quantitative nontreponemal serum antibody test (eg, rapid plasma reagin [RPR], Venereal Disease Research Laboratory [VDRL]); cord blood is not used for serum testing because results are less sensitive and specific. The placenta or umbilical cord should be analyzed using darkfield microscopy or fluorescent antibody staining if available.
Infants and young children with clinical signs of illness or suggestive serologic test results also should have a lumbar puncture with CSF analysis for cell count, VDRL, and protein; complete blood count (CBC) with platelet count; liver tests; long-bone radiographs; and other tests as clinically indicated (ophthalmologic evaluation, chest radiographs, neuroimaging, and auditory brain stem response).
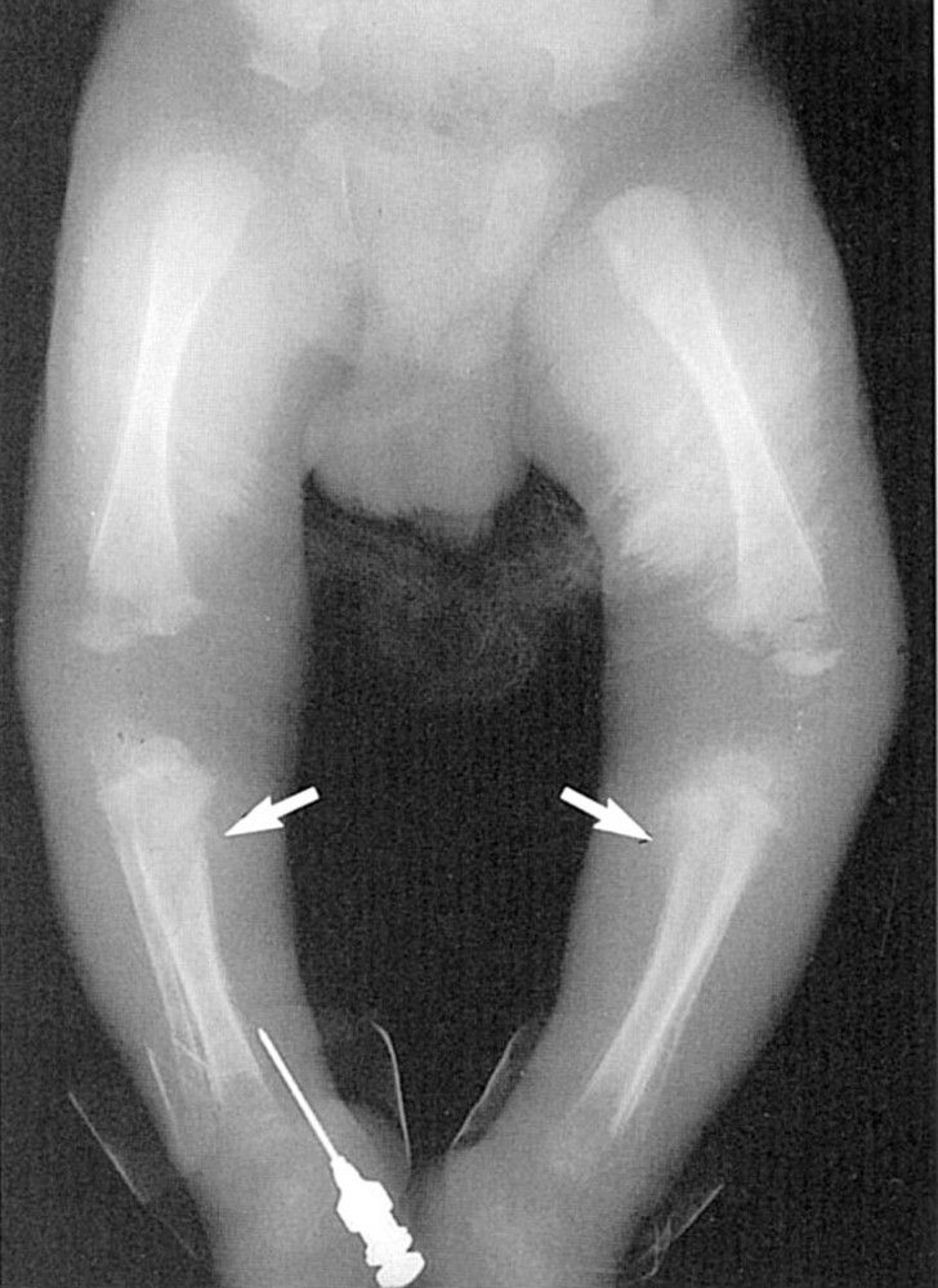
Syphilis can cause many different abnormalities on long-bone radiographs, including
Periosteal reactions
Diffuse or localized osteitis
Metaphysitis
The osteitis is sometimes described as diffuse "moth-eaten" changes of the shaft. Metaphysitis commonly appears as lucent or dense bands that can alternate to give a sandwich or celery stalk appearance. The Wimberger sign is symmetric erosions of the medial proximal tibia, but there can also be erosions in the metaphysis of other long bones. Excessive callus formation at the ends of long bones has been described. Many affected infants have more than one of these findings.

© Springer Science+Business Media
Diagnosis is confirmed by microscopic visualization of spirochetes in samples from the neonate or the placenta. Diagnosis based on neonatal serologic testing is complicated by the transplacental transfer of maternal IgG antibodies, which can cause a positive test in the absence of infection. However, a neonatal nontreponemal antibody titer > 4 times the maternal titer would not typically result from passive transfer, and diagnosis is considered confirmed or highly probable. Maternal disease acquired late in pregnancy may be transmitted before development of antibodies. Thus, in neonates with lower titers but typical clinical manifestations, syphilis is also considered highly probable. In neonates with no signs of illness and low or negative serologic titers, syphilis is considered possible; subsequent approach depends on various maternal and neonatal factors (see Follow up).
The utility of fluorescent assays for antitreponemal IgM, which is not transferred across the placenta, is controversial, but such assays have been used to detect neonatal infection. Any positive nontreponemal test should be confirmed with a specific treponemal test to exclude false-positive results, but confirmative testing should not delay treatment in a symptomatic infant or in an infant at high risk of infection.
Late congenital syphilis
Diagnosis of late congenital syphilis is by clinical history, distinctive physical examination findings, and positive serologic tests (see also Diagnostic tests for syphilis).
The Hutchinson triad of interstitial keratitis, Hutchinson incisors, and 8th cranial nerve deafness is diagnostic. Sometimes the standard nontreponemal serologic tests for syphilis (VDRL and RPR) are negative, but the fluorescent treponemal antibody absorption test (FTA-ABS) is positive. The diagnosis should be considered in cases of unexplained deafness, progressive intellectual deterioration, or keratitis.
Follow up
All seropositive infants and those whose mothers were seropositive should have nontreponemal antibody titers measured every 2 to 3 months until the test is nonreactive or the titer has decreased 4-fold. In uninfected and successfully treated infants, nontreponemal antibody titers are usually nonreactive by 6 months. Passively acquired treponemal antibodies may be present for longer, perhaps 15 months. It is important to remember to use the same specific nontreponemal test to monitor titers in mothers, neonates, infants, and young children over time.
If nontreponemal tests remain reactive past 6 to 12 months of age or titers increase, the infant should be reevaluated, including lumbar puncture for CSF analysis, complete blood count with platelet count, long-bone radiographs, and other tests as clinically indicated.
Treatment of Congenital Syphilis
Parenteral penicillin
Prenatal management
Pregnant patients in the early stages of syphilis receive a single dose of benzathine penicillin G (benzathine benzylpenicillin is used in some countries and in the United States if benzathine penicillin G is not available) (Pregnant patients in the early stages of syphilis receive a single dose of benzathine penicillin G (benzathine benzylpenicillin is used in some countries and in the United States if benzathine penicillin G is not available) (1). For later stages of syphilis or neurosyphilis, the appropriate regimen for nonpregnant patients should be followed (see Late latent or tertiary syphilis). Occasionally, a severe Jarisch-Herxheimer reaction occurs after such therapy, leading to spontaneous abortion. Patients allergic to penicillin may be desensitized and then treated with penicillin.
An ultrasound should performed when syphilis is diagnosed in the second half of pregnancy and a second dose of penicillin may be beneficial if fetal abnormalities are found.
After adequate treatment, nontreponemal test results decrease 4-fold by 6 to 12 months in most patients and revert to negative by 2 years in nearly all patients. Treatment failure or reinfection should be considered in patients who have a ≥ 4-fold increase in titers after treatment that is sustained for > 2 weeks.
Erythromycin therapy is inadequate for both the mother and fetus and is not recommended. Erythromycin therapy is inadequate for both the mother and fetus and is not recommended.Tetracycline is contraindicated.Tetracycline is contraindicated.
Early congenital syphilis
Treatment is indicated for infants with confirmed or highly probable syphilis and for infants with possible syphilis if a mother with confirmed or possible syphilis fits any of the following criteria:
Untreated
Treatment status unknown
Treated < 30 days before delivery
Inadequately treated (a nonpenicillin regimen)
Maternal evidence of relapse or reinfection (≥ 4-fold increase in maternal titer)
Partner recently diagnosed with syphilis
The 2021 Centers for Disease Control and Prevention (CDC) STI treatment guidelines recommend aqueous crystalline penicillin G IV or procaine penicillin G IM for 10 days. If ≥ 1 day of therapy is missed, the entire course must be repeated. In infants with possible syphilis whose mothers were not adequately treated but who are clinically well and have a completely negative full evaluation, a single dose of benzathine penicillin IM is an alternative treatment choice in selected circumstances but only if all components of the evaluation are negative and follow-up is ensured (recommend aqueous crystalline penicillin G IV or procaine penicillin G IM for 10 days. If ≥ 1 day of therapy is missed, the entire course must be repeated. In infants with possible syphilis whose mothers were not adequately treated but who are clinically well and have a completely negative full evaluation, a single dose of benzathine penicillin IM is an alternative treatment choice in selected circumstances but only if all components of the evaluation are negative and follow-up is ensured (2).
Older infants and children with newly diagnosed congenital syphilis
CSF should be examined before treatment starts. The CDC recommends that any child with late congenital syphilis be treated with aqueous crystalline penicillin GIV for 10 days. A single dose of benzathine penicillin G IM may also be given at the completion of the IV therapy. Alternatively, if a full evaluation is completely negative and the child is asymptomatic, benzathine penicillin G IM once a week for 3 weeks may be used. CSF should be examined before treatment starts. The CDC recommends that any child with late congenital syphilis be treated with aqueous crystalline penicillin GIV for 10 days. A single dose of benzathine penicillin G IM may also be given at the completion of the IV therapy. Alternatively, if a full evaluation is completely negative and the child is asymptomatic, benzathine penicillin G IM once a week for 3 weeks may be used.
Many patients do not revert to seronegativity but do have a 4-fold decrease in titer of reagin (eg, VDRL) antibody. Patients should have follow-up and testing performed every 3 months to ensure the appropriate serologic response to therapy has occurred and that there is no indication of relapse. Patients who do not have a 4-fold decrease after 12 to 18 months should be evaluated for neurosyphilis with CSF analysis and retreated.
Interstitial keratitis is usually treated with corticosteroid and atropine drops in consultation with an ophthalmologist. Patients with sensorineural hearing loss should be treated in collaboration with an otolaryngologist and may benefit from penicillin plus a corticosteroid. Corticosteroids have not been critically evaluated in these conditions. Interstitial keratitis is usually treated with corticosteroid and atropine drops in consultation with an ophthalmologist. Patients with sensorineural hearing loss should be treated in collaboration with an otolaryngologist and may benefit from penicillin plus a corticosteroid. Corticosteroids have not been critically evaluated in these conditions.
Treatment references
1. American College of Obstetricians and Gynecologists: Screening for Syphilis in Pregnancy, Practice Advisory. April 2024.
2. Centers for Disease Control and Prevention (CDC): Sexually Transmitted Infections Treatment Guidelines 2021. Congenital Syphilis.
Prevention of Congenital Syphilis
Pregnant patients should be routinely tested for syphilis at the first prenatal visit and, if they live in a community with high rates of syphilis or have any risk factors for syphilis, retested in the third trimester and at delivery (1). In the vast majority of cases, adequate treatment during pregnancy cures both mother and fetus. However, in some cases, syphilis treatment late in pregnancy eliminates the infection but not some signs of syphilis that appear at birth. Treatment of the mother < 4 weeks before delivery may not eradicate fetal infection.
When congenital syphilis is diagnosed, other family members should be examined for physical and serologic evidence of infection. Retreatment of the mother in subsequent pregnancies is necessary only if serologic titers suggest relapse or reinfection. Women who remain seropositive after adequate treatment may have been reinfected and should be reevaluated. A mother without lesions who is seronegative but who has had sexual contact with a person known to have syphilis should be treated because there is a high chance that she acquired syphilis.
Prevention reference
1. Centers for Disease Control and Prevention (CDC): Sexually Transmitted Diseases: State Statutory and Regulatory Language Regarding Prenatal Syphilis Screenings in the United States. Accessed December 12, 2024.
Key Points
Clinical manifestations of syphilis are classified as early congenital (birth through age 2 years) and late congenital (after age 2 years).
If syphilis is untreated during pregnancy, risk of transmission of maternal primary or secondary syphilis is high (> 60%); risk of transmission of untreated latent or tertiary syphilis is lower (< 40%).
Diagnose clinically and by serologic testing of mother and child; darkfield microscopy of skin lesions and sometimes of placenta and umbilical cord samples may help diagnose early congenital syphilis.
Treat with parenteral penicillin.







